“Individuals with Type 1 diabetes have an insulin PRODUCTION problem. They no longer produce insulin. However, individuals with type 2 diabetes have an insulin RESISTANCE problem. They produce insulin or some insulin, but their body resists its “commands or effects.”
How Normal Glucose Metabolism Works
- When you eat foods with carbohydrates, the carbs are broken down into individual particles called glucose (sugar).
- This sugar then goes to the bloodstream. We need to have some sugar circulating in our bloodstream, but not too much. After all, sugar is our primary source of energy.
- From the bloodstream, insulin (a hormone) carries (escorts) the excess sugar from the bloodstream inside the cells (muscle cells) to be used as energy (See image below).
Figure 1: Insulin acts like a “key,” opening the “door” of the cells for glucose to enter and be used as energy
.
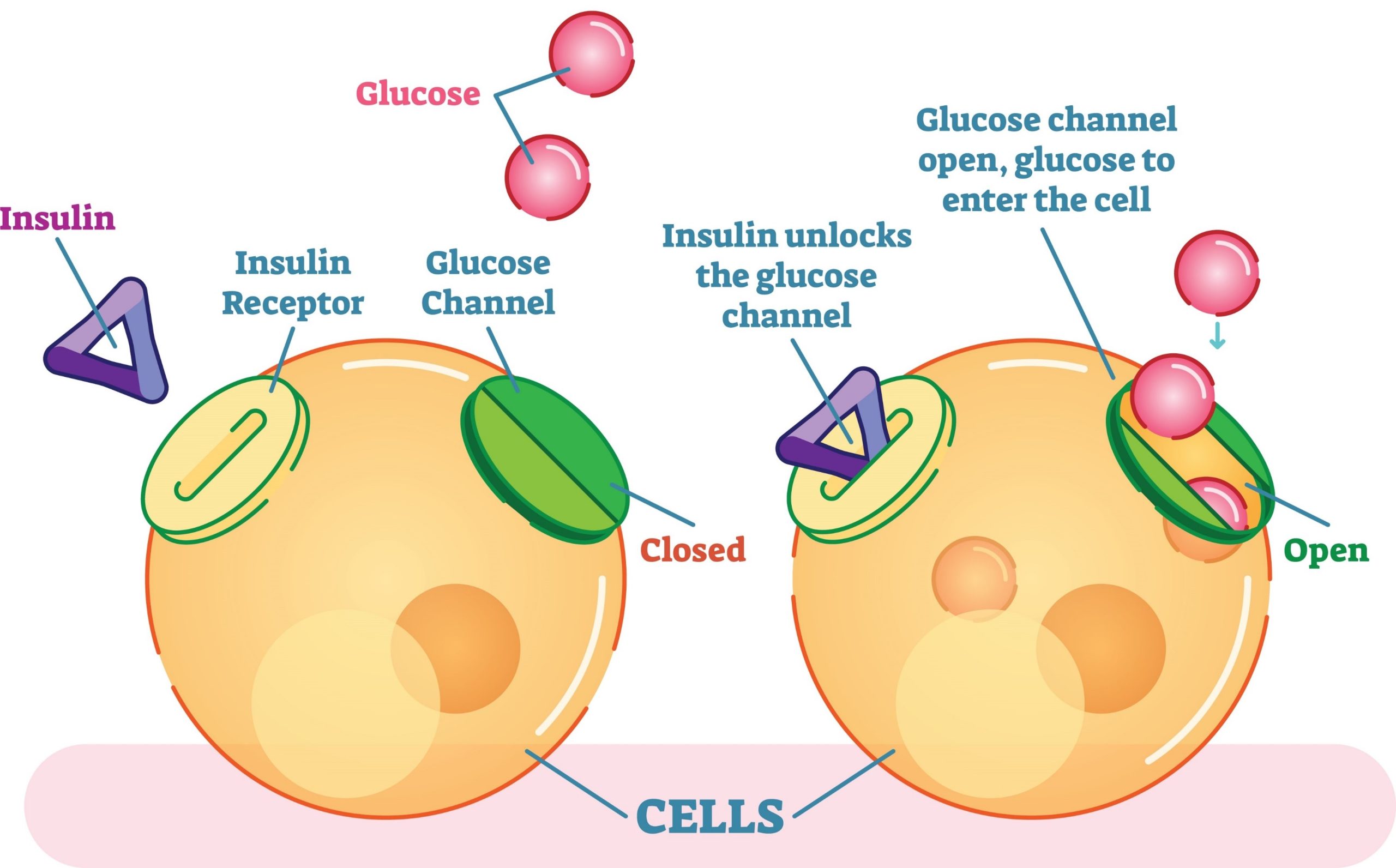
Retrieved from: GettyImages-904816340
Understanding Insulin Resistance
Type 2 diabetes represents more than 90% of all diabetes cases. It all starts with INSULIN RESISTANCE. If you were diagnosed with pre-diabetes, that means you are insulin-resistant. To understand what that means, imagine the figure above differently: insulin connects to the receptor “lock,” but the “door” will not open. THE CELL IS RESISTING TO OPEN THE DOOR! This is INSULIN RESISTANCE! Insulin commands the cell to open the door, but the cell resists its commands/effects. If the cell will not open the door, sugar cannot go into the cell. Sugar will be floating in the bloodstream, increasing the blood sugar. But here is the million-dollar question: Why is the cell not opening the door and resisting the insulin commands in the first place? It turns out there is an issue with the “lock.” The lock is “gummed up” with FAT! Yes, fat impairs insulin from working properly due to lipotoxicity, especially the saturated fat from the diet, bloodstream, and body fat storage. Researchers followed saturated fat using an MRI machine, and after a high-fat meal, the MRI showed fat going from the blood to the muscle. After 2 hours and 40 minutes of the high-fat meal, insulin could not work well! Thus, the underlying cause of insulin resistance in diabetes type 2 is fat clogging the cells. The “doors” cannot open, and as a consequence, the individual ends up with high blood sugar. High blood sugar is a symptom and not the cause of diabetes type 2.
The Relationship Between Obesity and Insulin Resistance
Obesity increases one’s risk of developing heart disease, cancer, type 2 diabetes, and other top-killer chronic conditions(Pi-Sunyer X, 2009). Likewise, in adults, childhood obesity leads to chronic diseases in adulthood, such as type 2 diabetes and heart disease (Kelsey et al., 2014). Visceral fat (fat around the organs or waist) is a great predictor, if not the greatest, of type 2 diabetes (Raheem et al., 2022), and up to 90% of individuals with diabetes are overweight (Ginter & Simko, 2012). Reducing belly fat/visceral fat is the best way to prevent prediabetes from turning into full-blown diabetes. This data indicates that weight loss is a critical component in reversing insulin resistance and becoming more sensitive to insulin. There is also a phenomenon called the spillover effect of obesity, where the fat cells (adipocytes) store so much fat that the cell membrane breaks up, releasing its fat content in the surrounding tissues. This effect causes both inflammation and insulin resistance. Obesity and diabetes are inflammatory conditions, but fortunately, they can be reversed. Obesity comes at a great cost to public health, the U.S. health system, and the individuals diagnosed with the condition. In 2008, the indirect and direct cost of obesity in the U.S. was $147B (Finkelstein et al., 2009). Diabetes costs around $16,752 per person diagnosed per year in the United States (ADA, n.a.). The greatest cost, however, is premature death, as heart disease is the top cause of premature death among individuals with diabetes.
Figure 2: The difference between visceral and subcutaneous fat
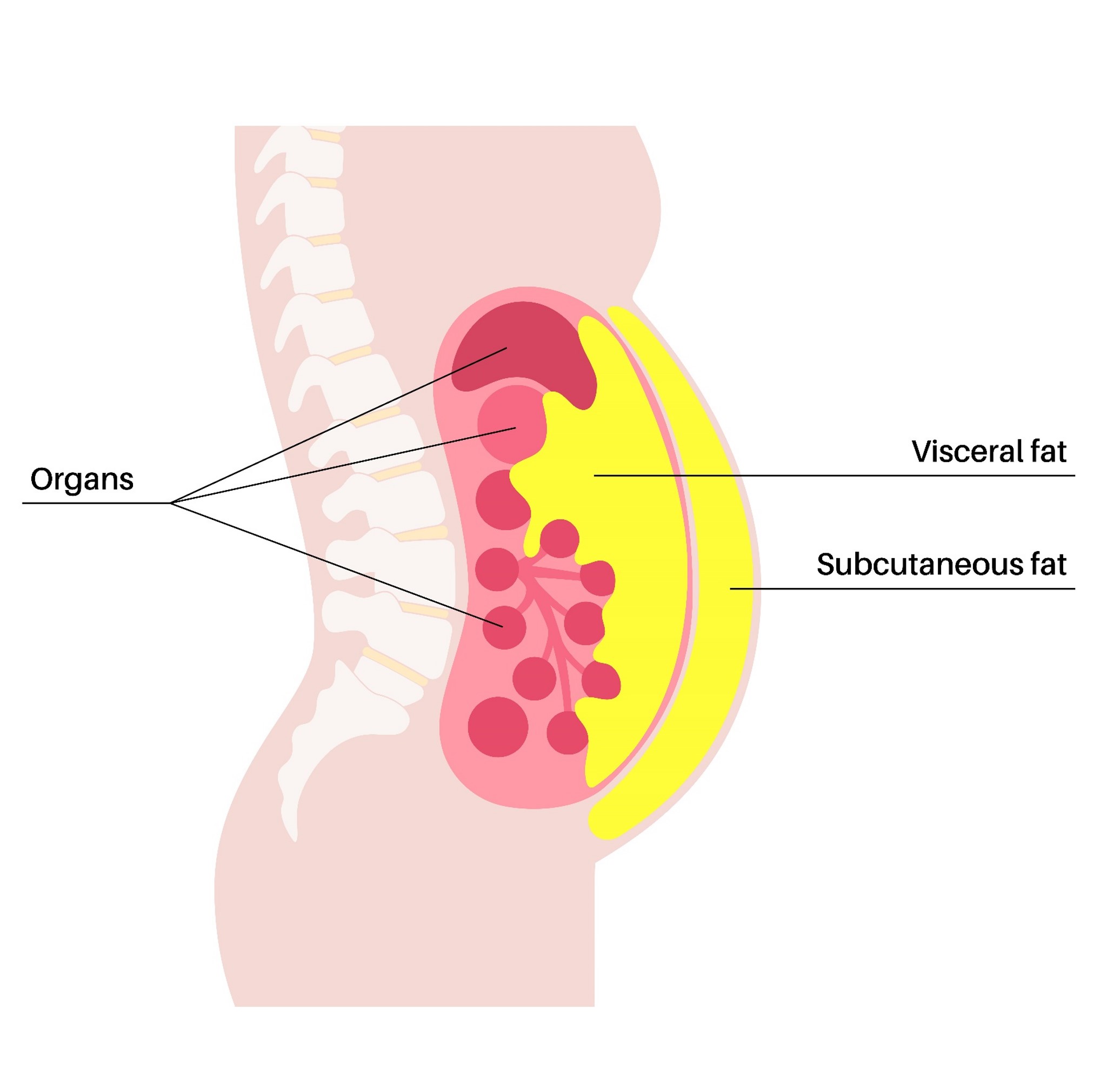
Getty Images – 1499582428
How to Reduce or Even Reverse Insulin Resistance
Understanding the root cause of insulin resistance (fat) is the key to reversing it. The reversal process of being insulin resistant is becoming insulin SENSITIVE! The benefits of becoming insulin sensitive are that your A1C levels can decrease to normal levels (no longer diabetic), and if you are a Type 1 diabetic, your insulin requirements can be reduced. It is well established for many years that type 2 diabetes can be reversed in many cases with only diet and lifestyle by reversing insulin resistance (Roden et al., 1996; Santomauro et al., 1999; Petersen et al., 2004; Taylor, R., 2008; Dunaief, et al., 2012; Kitessa & Abeywardena, 2016). A 5% weight loss increases insulin sensitivity and reduces the odds of developing chronic diseases, such as cardiovascular disease (Magkos et al., 2016). This modest weight loss also reduces hospitalizations and medication costs associated with diabetes (Espeland et al., 2014). If you are overweight or obese, reducing 1/5 of your body weight has been shown to reverse diabetes. Once you start losing weight, your body burns the visceral fat first! Weight loss is the most effective approach to reversing insulin resistance. Normal-weight individuals can also develop insulin resistance, but represent a smaller proportion of all individuals with diabetes. The reason is the same, fat inside the muscle cell clogging the ‘locks”.
The Wisest Way to Lose Weight
Technically, you can lose weight by any means, or through most types of diets promoting calorie restriction, but that does not mean it is the long-term, most healthful, or most sustainable way of losing weight. Most people become obsessed with calorie counting and portion control. These are important techniques, – but you can do more. Many reduce their meals to one or two per day. Well, for how long can they endure that? Feeling hungry and unsatisfied is not easy. Here is my solution: How about losing weight without tracking all the calories you eat during the day, without obsessing over portion control, or feeling hungry? Keep posted on my blogs, where I will write blogs about weight management. For now, here is my advice in a nutshell: Lose weight by eating MORE WHOLE PLANT FOODS! I mean legumes (beans and lentils), fruits, vegetables, whole grains, nuts, and seeds. Why?
- Whole plant foods are the only sources of fiber (which fills you up, removes excess bad fat from your body, reduces inflammation, controls blood sugar, feeds your gut bacteria, reduces leaky gut.)
- Whole plant foods are the only sources of powerful antioxidants (which will reduce inflammation related to diabetes and obesity).
- Whole plant foods are low in calories and high in water (you can eat these foods until you feel satiated because the fiber will absorb excess calories).
- Whole plant foods are low in saturated fats (except for coconut and palm oil)
- Whole plant foods have ZERO cholesterol.
- Whole plant foods are packed with vitamins and minerals to restore your health.
- Most whole plant foods have a low to moderate glycemic index, meaning they will not raise your blood sugar too fast. Please refer to my blog on how to increase fiber in white potatoes.
Note: Avoid consuming oil in excess.
Genetics vs. Epigenetics
Here is the good news: Genetics are only responsible for 20% of all diseases. Diabetes type 2 and obesity are considered lifestyle diseases. That means you have great control over these conditions. They are preventable, manageable, and, most importantly, reversible. Lifestyle is much more potent than genetics in determining the onset of these conditions. Many times people say these conditions “runs in the family”. If we look deeper, families usually share the same lifestyle and food habits, and if the lifestyle is not health-promoting, they will most likely share the same diseases. This is epigenetics, and epigenetics trumps genetics. In other words, genetics loads the gun (predisposition), but lifestyle (epigenetics) will ultimately either trigger the gun (genes) or not.
References
American Diabetes Association. (n.a). Life with Diabetes: The cost of diabetes. Retrieved from: https://diabetes.org/living-with-diabetes/financial-impact#:~:text=People%20with%20diagnosed%20diabetes%20incur,in%20the%20absence%20of%20diabetes.
Dunaief, D. M., Fuhrman, J., Dunaief, L. J., & Ying, G. (2012). Glycemic and cardiovascular parameters improved in type 2 diabetes with the high nutrient density (HND) diet. Open Journal of Preventive Medicine. 2(3), doi:10.4236/ojpm.2012.23053
Espeland, M. A., Glick, H. A., Bertoni, A., Brancati, F. L., Bray, G. A., Clark, J. M., Curtis, J. M., Egan, C., Evans, M., Foreyt, J. P., Ghazarian, S., Gregg, E. W., Hazuda, H. P., Hill, J. O., Hire, D., Horton, E. S., Hubbard, V. S.,
Finkelstein, E. A, Trogdon, J. G, Cohen, J. W. & Dietz, W. (2009). Annual medical spending attributable to obesity: Payer-and service-specific estimates. Health Affairs, (5), 822-831. doi:10.1377/hlthaff.28.5.w822.
Ginter, E., & Simko, V. (2012). Type 2 diabetes mellitus, pandemic in 21st century. Advances in experimental medicine and biology, 771, 42–50. https://doi.org/10.1007/978-1-4614-5441-0_6
Kelsey, M. M., Zaepfel, A., Bjornstad, P., & Nadeau, K. J. (2014). Age-related consequences of childhood obesity. Gerontology, 60(3), 222–228. https://doi.org/10.1159/000356023
Kitessa, S., & Abeywardena, M. (2016). Lipid-Induced Insulin Resistance in Skeletal Muscle: The Chase for the Culprit Goes from Total Intramuscular Fat to Lipid Intermediates, and Finally to Species of Lipid Intermediates. Nutrients, 8(8), 466. http://dx.doi.org/10.3390/nu8080466
Magkos, F., Fraterrigo, G., Yoshino, J., Luecking, C., Kirbach, K., Kelly, S. C., de Las Fuentes, L., He, S., Okunade, A. L., Patterson, B. W., & Klein, S. (2016). Effects of Moderate and Subsequent Progressive Weight Loss on Metabolic Function and Adipose Tissue Biology in Humans with Obesity. Cell metabolism, 23(4), 591–601. https://doi.org/10.1016/j.cmet.2016.02.005
Petersen, K. F., Dufour, S., Befroy, D., Garcia, R., & Shulman, G. I. (2004). Impaired mitochondrial activity in the insulin-resistant offspring of patients with type 2 diabetes. The New England Journal of Medicine, 350(7), 664–671. https://doi.org/10.1056/NEJMoa031314
Pi-Sunyer X. (2009). The medical risks of obesity. Postgraduate Medicine, 121(6), 21–33. https://doi.org/10.3810/pgm.2009.11.2074
Raheem, J., Sliz, E., Shin, J., Holmes, M. V., Pike, G. B., Richer, L., Gaudet, D., Paus, T., & Pausova, Z. (2022). Visceral adiposity is associated with metabolic profiles predictive of type 2 diabetes and myocardial infarction. Communications Medicine, 2, 81. https://doi.org/10.1038/s43856-022-00140-5
Roden, M., Price, T. B., Perseghin, G., Petersen, K. F., Rothman, D. L., Cline, G. W., & Shulman, G. I. (1996). Mechanism of free fatty acid-induced insulin resistance in humans. The Journal of Clinical Investigation, 97(12), 2859–2865. https://doi.org/10.1172/JCI118742
Santomauro, A. T., Boden, G., Silva, M. E., Rocha, D. M., Santos, R. F., Ursich, M. J., Strassmann, P. G., & Wajchenberg, B. L. (1999). Overnight lowering of free fatty acids with Acipimox improves insulin resistance and glucose tolerance in obese diabetic and nondiabetic subjects. Diabetes, 48(9), 1836–1841. https://doi.org/10.2337/diabetes.48.9.1836
Taylor R. (2008). Pathogenesis of type 2 diabetes: tracing the reverse route from cure to cause. Diabetologia, 51(10), 1781–1789. https://doi.org/10.1007/s00125-008-1116-7
 20
20
